Thoracic Support Driving: Posture Activator™ or Posture Inhibitor™?
by Dennis Zacharkow, PT
© 2015
Whether or not thoracic support optimizes one’s driving posture depends on the specific location of the thoracic support.
-
Correcting a Slumped Driving Posture
The main cause of a slumped driving posture is the hinging forward and downward of the rib cage due to flexion of the lower thoracic spine.1,2 The lower thoracic spine (just below the shoulder blades) is the “hinge area” for spinal flexion.3-9 (See Figure 1.)
 Figure 1:
Figure 1:
Circle denotes area of the thoracic spine responsible for the hinging forward and downward of the rib cage. Adapted from Bennett, H.E.: School Posture and Seating. Boston, Ginn and Company, 1928.Correcting a slumped driving posture requires firm, isolated support to only the lower thoracic spine (T10-T12). This lower thoracic support will elevate and stabilize the rib cage, and elongate the spine. Head, neck, and shoulder posture will all be dramatically improved through firm, isolated support to the lower thoracic spine.
Support above the lower thoracic spine to the mid-thoracic and upper thoracic spinal regions cannot correct the hinging forward and downward of the rib cage. Support at the mid-thoracic and/or upper thoracic levels will only push the upper back and shoulders forward, without being able to elevate the rib cage.
So, the corrective postural force must be localized to just the lower thoracic spine and no higher to effectively elevate the rib cage and correct a slumped driving posture.
Lower Thoracic Support = Posture Activator (See Figure 2.)
Mid-Thoracic Support = Posture Inhibitor
Upper Thoracic Support = Posture Inhibitor
Full Thoracic Support (Lower + Mid + Upper) = Posture Inhibitor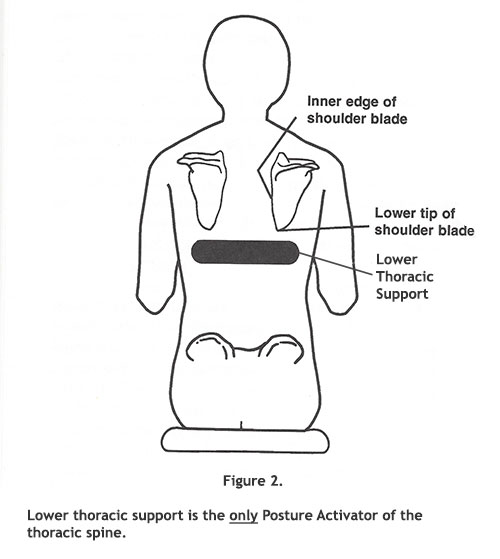
-
Optimizing Diaphragmatic Breathing
With a slumped driving posture, diaphragmatic breathing is restricted, and upper chest breathing predominates. This leads to shallow inspiration and a chronic state of fatigue.
The firm pressure from a lower thoracic support against the T10-T12 region of the back when driving immediately promotes proper diaphragmatic breathing by eliciting the intercostal-to-phrenic reflexes.10,11 (This occurs because the nerve connected to the diaphragm muscle, the phrenic nerve, is under the control of reflexes that are activated by pressure stimulation of other nerves in the region of the lower thoracic spine.)
In contrast to pressure stimulation against the T10-T12 region promoting proper diaphragmatic breathing, pressure stimulation at the mid-thoracic level (T5-T6) impairs diaphragmatic breathing by inhibiting these same reflexes.12,13
-
Proper Shoulder Blade Positioning
Lower thoracic support is located just below the shoulder blades (scapulae). By not applying pressure to the shoulder blades, lower thoracic support facilitates the proper positioning of the shoulder blades, which should lie “flat and widened across the back of the properly expanded chest.”14
In contrast, support to the mid-thoracic and/or the upper thoracic spine applies direct pressure to the shoulder blades. This abnormal pressure stimulation leads to a rounding of the back and shoulders.
A narrow and vertical, full thoracic support avoids pressure on the shoulder blades. However, besides not correcting a slumped driving posture and not optimizing diaphragmatic breathing, these narrow, vertical supports destabilize one’s posture when making turns with the vehicle.
These narrow, vertical supports can also distort one’s shoulder blade posture if the driver is instructed (as frequently occurs with many health professionals) to “pull the shoulders back.” This movement will prevent an elongated driving posture by retracting instead of widening the shoulder blades. Maintaining this distorted shoulder posture will quickly fatigue the upper back and neck.15
Some health professionals recommend placing a vertical thoracic support directly behind the sternum (breastbone) to elevate the rib cage. However, the length of the sternum corresponds to vertebral levels T2 through T9.16 So, support behind the sternum is only upper and mid-thoracic support, and is located too high to elevate the rib cage.
-
Combining Lower Thoracic Support with Sacral Support
There are only 2 Posture Activators for promoting an elongated driving posture: Lower Thoracic Support and Sacral Support. They must always be applied together.
By itself, sacral support will stabilize the pelvis, but it will not correct the hinging forward and downward of the rib cage.
By itself, lower thoracic support will elevate the rib cage, but it will not stabilize the pelvis. This lack of pelvic stabilization is the greatest risk factor for developing a herniated lumbar disc from driving.17
Health professionals advocating thick thoracic supports, but no accompanying sacral support, are greatly increasing their clients’ pelvic instability when driving, and greatly increasing their clients’ risk for developing a herniated lumbar disc.
Lower Thoracic Support and Sacral Support should also never be combined with the most prevalent of all Posture Inhibitors – Lumbar Support!18
References
- Zacharkow, D.: Posture: Sitting, Standing, Chair Design and Exercise. Springfield, Thomas, 1988.
- Zacharkow, D.: ZACKBACK Sitting. Rochester, ZACKBACK International, 1998.
- Latham, F.: A study in body ballistics: seat ejection. Proceedings of the Royal Society of London, Series B, 147:121-139, 1957.
- Rathbone, J.L.: Corrective Physical Education. Philadelphia, Saunders, 1934.
- Humphry, G.M.: A Treatise on the Human Skeleton. Cambridge, MacMillan, 1858.
- Vulcan, A.P., King, A.I., and Nakamura, G.S.: Effects of bending on the vertebral column during +Gz acceleration. Aerospace Medicine, 41:294-300, 1970.
- Alexander, C.J.: Scheuermann’s disease. Skeletal Radiology. 1:209-221, 1977.
- Markolf, K.L.: Deformation of the thoracolumbar intervertebral joints in response to external loads. The Journal of Bone and Joint Surgery, 54-A:511-533, 1972.
- White, A.A., and Panjabi, M.M.: Clinical Biomechanics of the Spine. Philadelphia, Lippincott, 1978, p.84.
- Decima, E.E., von Euler, C., and Thoden, U.: Intercostal-to-phrenic reflexes in the spinal cat. Acta Physiologica Scandinavica, 75:568-579, 1969.
- Leanderson R., Sundberg, J., and von Euler, C.: Role of diaphragmatic activity during singing: a study of transdiaphragmatic pressures. Journal of Applied Physiology, 62:259-270, 1987.
- Romaniuk, J.R., Supinski, G.S., and DiMarco, A.F.: Reflex control of diaphragm activation by thoracic afferents. Journal of Applied Physiology, 75:63-69, 1993.
- Remmers, J.E.: Extra-segmental reflexes derived from intercostal afferents: phrenic and laryngeal responses. Journal of Physiology, 233:45-62, 1973.
- Barlow, W.: The Alexander Technique. New York, Warner, 1980.
- Zacharkow, D.: Round Shoulders Misconceptions. (Available online.)
- Basmajian, J.V.: Surface Anatomy. An Instruction Manual. Baltimore, Williams and Wilkins, 1977.
- Zacharkow, D.: Driving with Sacral Support: The Key to Preventing a Herniated Lumbar Disc. March 2013. (Available online.)
- Zacharkow, D.: 3 Reasons to Avoid Driving with Lumbar Support. October 2015. (Available online.)